
Under the proposed expansion of Medi-Cal to undocumented seniors, vulnerable Californians would gain comprehensive health insurance. The policy improves access to care for individual seniors and could alleviate the financial burden on counties that serve undocumented immigrants in indigent care programs, increasing resources for other low-income groups.
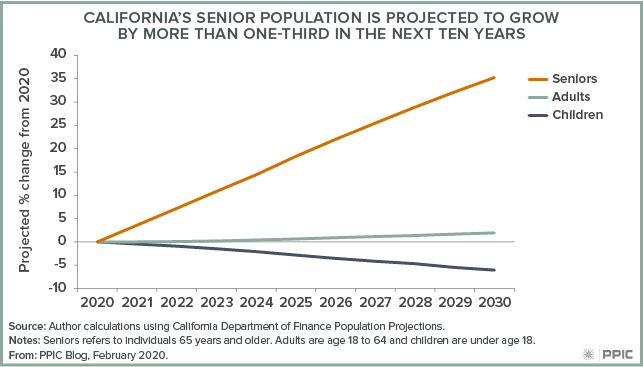
The senior population in California is projected to increase by over 2 million in the next decade, dramatically outpacing growth of younger groups in a demographic shift known as the Silver Tsunami. This increase, in particular among those in older age groups (75 to 84), will test California’s health care delivery and financing systems, because seniors are more likely to be disabled and to have complex or multiple health conditions than younger groups.
While most California seniors have health insurance—with Medicare being the most common—not all seniors have coverage. Many uninsured seniors are likely to be undocumented, making them ineligible for Medicare or to purchase coverage through Covered California, the state’s health insurance marketplace. These same seniors may have limited finances and therefore also are likely to struggle to access and afford health care.
Currently, most uninsured, undocumented seniors rely on safety net providers and a limited form of Medi-Cal that covers only emergencies, along with indigent care programs in certain counties that choose to cover undocumented immigrants. Under the expansion, these seniors would gain access to full-scope Medi-Cal, connecting them to preventive care and to programs to improve their disease management. Some expansion funds would also apply to the In-Home Supportive Services (IHSS) program, which pays for a caregiver—often a relative—to provide support for a senior to continue living at home rather than entering a costly long-term care facility.
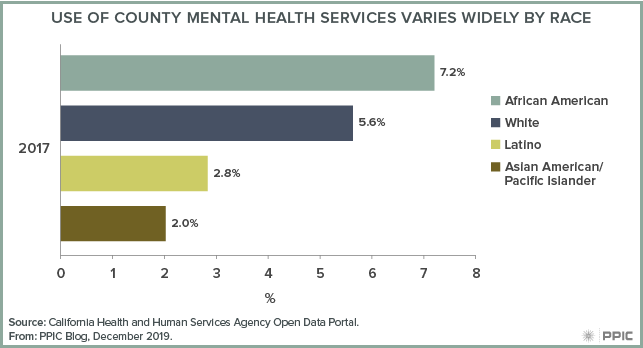
The budget estimates state costs of $320 million for the expansion, which would benefit 27,000 individuals. If enacted, the policy could have implications for local finances. Counties in California provide health care and mental health services to the medically indigent, with some areas—most notably Los Angeles—serving undocumented immigrants. These county programs, together with community clinics and emergency rooms, are essential access points to health care for undocumented, uninsured seniors. If undocumented seniors become eligible for full-scope Medi-Cal, the state would finance their care instead of the county, where applicable. This shift could free up funding that could then be invested in other health-related county responsibilities, such as disaster preparedness, prevention activities, and substance use disorder treatment.
A complicated fiscal relationship between the state and counties, however, makes it difficult to estimate how much funding could be redirected if this group of seniors gain access to Medi-Cal. As state lawmakers consider the policy change, it will be important to consider how it may affect local and state finances.








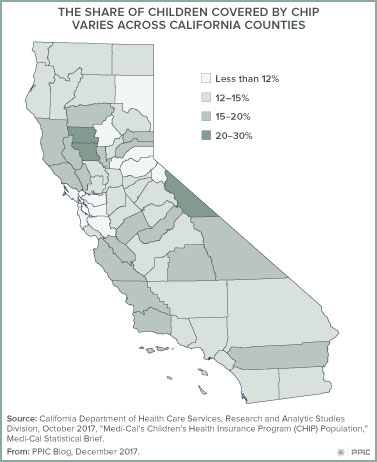 As of May 2017, a quarter of the more than 5.2 million California children covered by Medi-Cal (the state’s Medicaid program)
As of May 2017, a quarter of the more than 5.2 million California children covered by Medi-Cal (the state’s Medicaid program) 


