
Governor Newsom is proposing to expand access to Medi-Cal—the state’s Medicaid program—for low-income young adults up to age 26, regardless of their immigration status. This could help a vulnerable segment of the immigrant population. Californians are signaling broad support.
Overall, immigrants make up about 27% of the state’s population and are less likely to have health insurance than US-born Californians. Immigrants are also less likely to have private insurance, partly due to differences in employment industries and income.

Documented immigrants—including those with green cards and visas—may qualify for Medi-Cal without being subject to the five-year waiting period required by federal law. They can also purchase private health plans through Covered California, the health insurance exchange that was created as part of the Affordable Care Act (ACA). However, most recently-arrived elderly immigrants are not eligible for Medicare because they have not paid Medicare taxes over a long enough period.
California offers a patchwork of health care options for undocumented immigrants, who are not covered by the ACA. For instance, low-income children and pregnant residents are eligible for Medi-Cal regardless of immigration status, and some counties include undocumented immigrants in programs for those who cannot afford medical care. Additional options for undocumented immigrants include community clinics, rural health clinics, emergency rooms, or a limited version of Medi-Cal for medical emergencies.
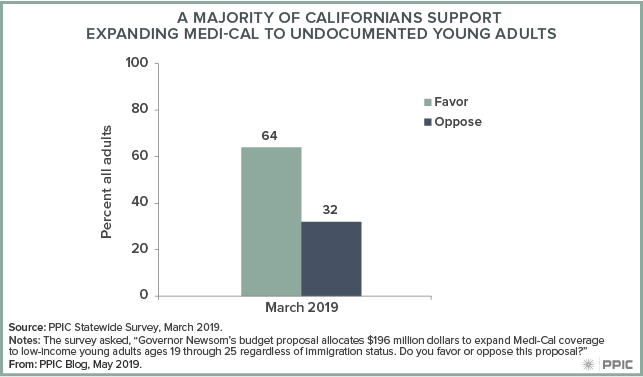
Californians support health care access for undocumented immigrants. In a 2015 PPIC Statewide Survey, a slim majority of Californians (54%) supported the idea of providing health care coverage to undocumented immigrants. In March 2019, about two-thirds (64%) expressed support for the governor’s proposed expansion of Medi-Cal coverage to low-income young adults, including those who are undocumented.
The governor’s May budget revision delays implementation of the expansion, but it would still have an impact: by providing coverage to approximately 90,000 undocumented young adults in the first year, it could help make the health care landscape less complicated for an important share of California’s immigrant population.










 Because highly disadvantaged young men are detached from educational and labor market institutions, they are likely to be among the hardest to reach through traditional sites of enrollment. They are also disproportionately represented among people who are arrested and incarcerated in county jails and state prisons.
Because highly disadvantaged young men are detached from educational and labor market institutions, they are likely to be among the hardest to reach through traditional sites of enrollment. They are also disproportionately represented among people who are arrested and incarcerated in county jails and state prisons.